Cancer remains a formidable public health challenge across the United States, with striking geographical variations that reveal complex patterns of disease distribution. The latest data from the Centers for Disease Control and Prevention shows significant disparities in cancer incidence rates between states, ranging from over 512 cases per 100,000 residents in Kentucky to fewer than 367 cases per 100,000 in New Mexico. These variations reflect a complex interplay of environmental, occupational, lifestyle, and socioeconomic factors that create distinct regional cancer burdens. Understanding these geographic patterns provides crucial insights for targeted prevention strategies, resource allocation, and public health interventions designed to address the underlying causes of cancer disparities across American communities.
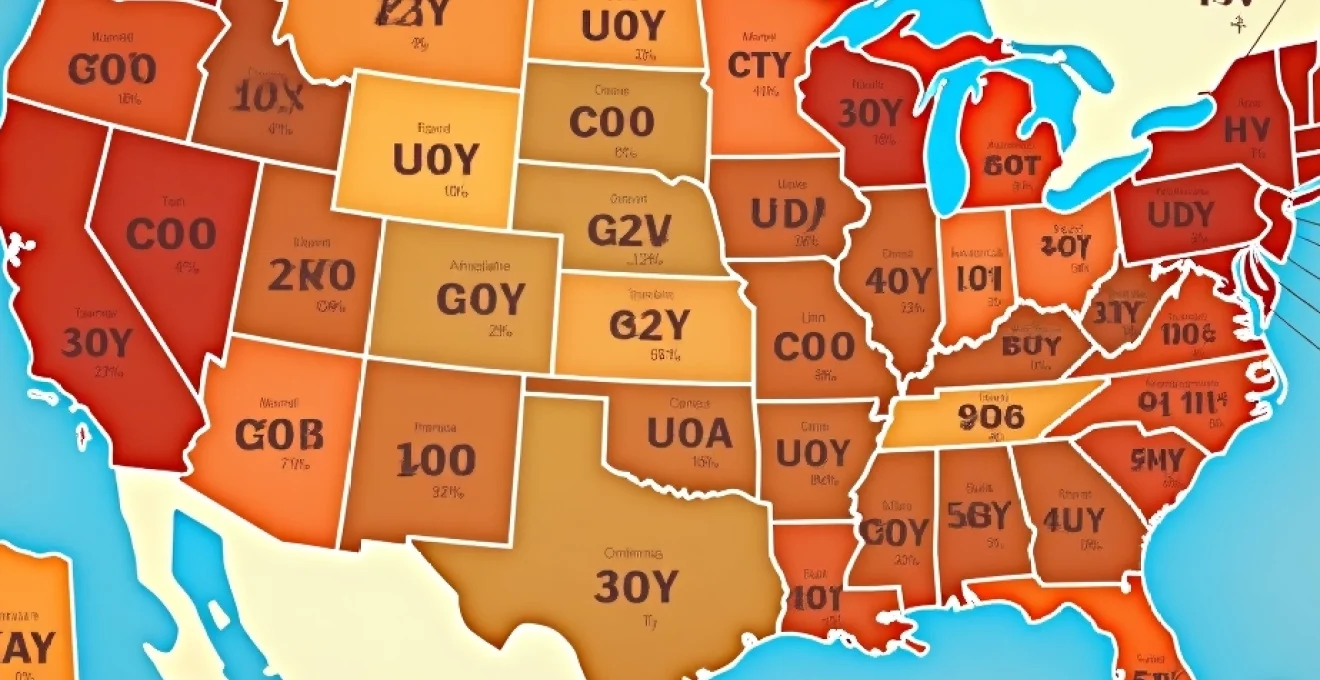
Age-standardised cancer incidence rates across US states
The geographic distribution of cancer rates across the United States reveals stark regional differences that have persisted for decades. According to the most recent comprehensive data analysis, Kentucky leads the nation with an age-adjusted cancer incidence rate of 512.0 cases per 100,000 residents, followed closely by West Virginia at 510.6 and Iowa at 505.9 cases per 100,000. These rates significantly exceed the national average of approximately 450 cases per 100,000 people, highlighting the disproportionate cancer burden faced by certain regions.
The southeastern and Appalachian regions consistently demonstrate elevated cancer incidence rates, with Louisiana, Mississippi, and Arkansas all ranking among the top ten states for new cancer diagnoses. This geographical clustering suggests common underlying risk factors that transcend state boundaries, including environmental exposures, cultural practices, and shared demographic characteristics. The persistence of these patterns over multiple years indicates that structural factors, rather than temporary fluctuations, drive these regional disparities.
Conversely, western and southwestern states typically report substantially lower cancer incidence rates. New Mexico consistently maintains the lowest cancer rate nationally at 366.9 cases per 100,000 residents, followed by Massachusetts at 377.9 and Colorado at 382.2. This 45% difference between the highest and lowest rates represents thousands of potential cancer cases that could be prevented through targeted interventions addressing the modifiable risk factors contributing to these disparities.
Kentucky’s Tobacco-Related malignancy prevalence
Kentucky’s position as the state with the highest overall cancer rate stems largely from its exceptionally high burden of tobacco-related malignancies. The state records 82.8 lung cancer cases per 100,000 residents annually, nearly 30 points above the national average of 54 cases per 100,000. This elevated rate directly correlates with Kentucky’s adult smoking prevalence, which ranks second-highest nationally, with tobacco use affecting approximately 23% of the adult population.
The tobacco connection extends beyond lung cancer to encompass multiple malignancy types. Kentucky ranks second nationally for pancreatic cancer rates and third for laryngeal cancer, both strongly associated with smoking. The state’s tobacco-growing heritage and cultural normalisation of smoking have created a persistent public health challenge that continues to manifest in elevated cancer statistics across multiple generations.
West virginia’s coal mining carcinogen exposure impact
West Virginia’s second-place ranking in national cancer incidence rates reflects the long-term health consequences of extensive coal mining operations and related industrial activities. The state’s cancer rate of 510.6 cases per 100,000 residents is particularly elevated for lung and bronchus cancers, which affect mining communities disproportionately. Coal miners face increased exposure to silica dust, diesel exhaust, and other known carcinogens during their occupational activities.
The geographic concentration of cancer cases in West Virginia’s coal-producing counties demonstrates clear environmental health impacts. Communities located near active or former mining operations show consistently higher cancer rates than state averages , suggesting that both occupational and community-wide environmental exposures contribute to the elevated disease burden. Additionally, the economic challenges facing former mining communities often result in limited access to preventive healthcare services and delayed diagnosis.
Louisiana’s petrochemical corridor cancer clusters
Louisiana’s cancer rate of 488.8 cases per 100,000 residents reflects significant environmental health challenges, particularly in the petrochemical corridor along the Mississippi River. This industrial region, sometimes referred to as “Cancer Alley,” hosts numerous petroleum refineries, chemical plants, and related facilities that release various carcinogenic compounds into the surrounding environment. The concentration of industrial facilities creates cumulative exposure risks for nearby communities.
Prostate cancer rates in Louisiana rank highest nationally at 148.9 cases per 100,000 residents, with African American men facing particularly elevated risks. The state’s large African American population experiences disproportionate cancer burdens due to both genetic predisposition and environmental justice issues that concentrate industrial pollution in predominantly minority communities. This intersection of demographic vulnerability and environmental hazards creates compounding health risks.
Delaware’s lung cancer mortality statistics
Despite its small size, Delaware ranks among the top states for cancer incidence with 459.8 cases per 100,000 residents. The state faces particular challenges with lung cancer mortality, attributed to both historical industrial exposures and current air quality issues. Delaware’s location within the heavily industrialised Mid-Atlantic corridor subjects residents to regional air pollution from multiple sources, including power plants, refineries, and transportation networks.
The state’s proximity to major metropolitan areas and industrial centers contributes to elevated background levels of airborne carcinogens. Additionally, Delaware’s historical shipbuilding and chemical industries have left legacies of occupational cancer risks that continue to manifest in current disease statistics. The cumulative impact of multiple exposure sources creates persistent cancer risk patterns that require comprehensive environmental health interventions.
Environmental carcinogen exposure patterns by geographic region
Regional environmental factors play crucial roles in determining cancer incidence patterns across different geographic areas of the United States. Industrial emissions, natural radiation sources, and environmental contamination create distinct exposure profiles that correlate strongly with observed cancer rate variations. The southeastern states, which consistently rank highest for cancer incidence, face multiple environmental challenges including industrial pollution, natural radon exposure, and climate-related factors that may influence carcinogen persistence and bioavailability.
Air quality measurements reveal significant regional variations in carcinogenic pollutant concentrations. The American Lung Association’s State of the Air report indicates that counties in Kentucky, West Virginia, and Louisiana frequently experience poor air quality days, with elevated levels of particulate matter and ozone that contribute to respiratory cancer risks. These environmental conditions create chronic exposure scenarios that accumulate over decades of residence in affected areas.
Environmental justice concerns arise when industrial facilities and pollution sources are disproportionately located in low-income communities and communities of colour, creating cumulative environmental health risks that contribute to cancer disparities.
Industrial chemical emissions in cancer alley louisiana
The 85-mile stretch of Louisiana’s Mississippi River corridor between New Orleans and Baton Rouge hosts over 200 petrochemical facilities that collectively emit millions of pounds of toxic chemicals annually. EPA Toxics Release Inventory data shows this region releases benzene, formaldehyde, ethylene oxide, and other known carcinogens at concentrations significantly exceeding national averages. Residents in this area face cancer risks up to 50 times higher than national averages according to EPA risk assessments.
Community-based epidemiological studies have documented elevated rates of multiple cancer types in parishes adjacent to major industrial facilities. The cumulative impact of multiple emission sources creates complex exposure mixtures that may have synergistic carcinogenic effects beyond what would be predicted from individual chemical assessments. Air monitoring data consistently shows elevated concentrations of volatile organic compounds and hazardous air pollutants in residential areas near these facilities.
Radon gas concentrations in appalachian mining communities
Natural radon gas exposure represents a significant environmental carcinogen source in Appalachian regions, particularly affecting Kentucky, West Virginia, and parts of Pennsylvania. Underground uranium deposits and geological formations in these areas create elevated background radon levels that contribute to lung cancer risks. The EPA estimates that radon exposure causes approximately 21,000 lung cancer deaths annually nationwide, with Appalachian communities experiencing disproportionate impacts.
Coal mining activities can disturb geological formations and increase radon release into residential areas. Former mining sites and underground workings may serve as conduits for radon gas migration into homes and buildings. The combination of occupational mining exposures and residential radon creates compounding lung cancer risks for mining community residents. Indoor radon testing reveals that many homes in these regions exceed EPA action levels requiring mitigation measures.
Agricultural pesticide usage in midwest cancer hotspots
Iowa’s third-place ranking for national cancer incidence reflects, in part, intensive agricultural chemical usage throughout the state’s farming regions. The state leads the nation in corn and soybean production, crops that receive substantial pesticide and herbicide applications during growing seasons. Atrazine, glyphosate, and other agricultural chemicals have been detected in groundwater and surface water sources throughout Iowa’s agricultural counties.
Epidemiological studies of farming communities show elevated rates of lymphomas, leukaemias, and brain cancers potentially associated with pesticide exposures. Agricultural workers face direct occupational exposures, while rural residents may experience indirect exposures through contaminated water sources and aerial drift during application periods. The temporal patterns of cancer diagnosis in farming communities often correspond with decades of cumulative pesticide exposure , suggesting long latency periods between exposure and disease development.
Air quality index correlations with respiratory malignancies
Metropolitan areas within high-cancer-rate states frequently experience poor air quality conditions that contribute to respiratory cancer burdens. The correlation between particulate matter concentrations and lung cancer incidence becomes apparent when examining county-level data within states like Kentucky, Louisiana, and West Virginia. Urban areas with multiple pollution sources, including traffic, industry, and power generation, create complex mixtures of airborne carcinogens.
Diesel exhaust particles, which are classified as definite human carcinogens, represent significant contributors to urban air pollution in industrial regions. Transportation corridors, shipping ports, and freight distribution centers generate substantial diesel emissions that affect surrounding communities. The interaction between multiple air pollution sources creates cumulative exposure risks that exceed the sum of individual source contributions, particularly affecting vulnerable populations including children and elderly residents.
Demographic risk factors and socioeconomic cancer disparities
Socioeconomic factors create substantial disparities in cancer incidence and outcomes across different states and communities. States with the highest cancer rates often coincide with regions experiencing elevated poverty rates, limited educational opportunities, and reduced access to healthcare services. Kentucky, Louisiana, Arkansas, West Virginia, and Mississippi—all ranking among the top states for cancer incidence—also represent five of the six states with the largest proportions of residents living below the poverty line.
The relationship between poverty and cancer risk operates through multiple pathways, including delayed medical care, inadequate preventive screening, poor nutrition, increased tobacco and alcohol use, and residence in environmentally compromised areas. Low-income communities often face greater exposure to environmental carcinogens due to housing proximity to industrial facilities, major transportation corridors, and other pollution sources. Additionally, economic constraints may limit individuals’ ability to relocate from high-risk areas or implement protective measures in their homes.
Educational attainment strongly correlates with cancer prevention behaviours and health outcomes. States with lower average educational levels tend to have higher smoking rates, lower screening participation, and delayed medical attention for symptoms. Health literacy challenges in these communities can impede understanding of cancer risk factors and prevention strategies , contributing to persistently elevated cancer rates. Cultural factors and community norms around health-seeking behaviour also influence cancer prevention and early detection practices.
Racial and ethnic disparities compound socioeconomic factors to create particularly severe cancer burdens for minority populations. African American men face prostate cancer rates nearly double those of white men, with Louisiana’s African American communities experiencing some of the highest rates nationally. Similarly, African American women have lower breast cancer incidence rates but higher mortality rates compared to white women, reflecting disparities in access to quality treatment and early detection services.
The intersection of race, poverty, and environmental exposure creates compounding cancer risks that require comprehensive interventions addressing social determinants of health alongside traditional medical approaches.
State-specific screening programme effectiveness and early detection rates
Cancer screening programme participation and effectiveness vary dramatically across states with different incidence rates, contributing to observed disparities in both diagnosis timing and survival outcomes. States with comprehensive screening programmes and high participation rates often demonstrate better cancer outcomes despite potentially elevated exposure risks. However, states with the highest cancer incidence frequently struggle with screening programme implementation due to healthcare infrastructure limitations, geographic barriers, and population-level factors affecting programme participation.
Mammography screening rates for breast cancer show substantial interstate variation, with some states achieving screening rates above 80% of eligible women while others fall below 70%. These differences translate directly into cancer outcomes, as early-stage breast cancer detection dramatically improves survival prospects. Similarly, colonoscopy screening for colorectal cancer varies from over 75% participation in some states to less than 65% in others, contributing to interstate differences in colorectal cancer mortality rates.
Cervical cancer screening through Pap tests demonstrates even greater interstate variation, with rural and impoverished communities facing particular challenges in programme access. States with robust public health infrastructure and adequate healthcare provider networks achieve higher screening participation , resulting in lower cervical cancer incidence and mortality rates. Mobile screening programmes and community health worker initiatives have shown promise in addressing geographic and access barriers in underserved areas.
Lung cancer screening programmes represent newer interventions with significant potential for reducing cancer mortality in high-incidence states. Low-dose computed tomography screening for high-risk individuals, particularly current and former smokers, can detect lung cancers at earlier, more treatable stages. However, programme implementation requires substantial healthcare infrastructure investments and patient education efforts that may be challenging in resource-limited communities.
Occupational hazard classifications contributing to regional cancer burdens
Occupational exposures to carcinogenic substances contribute significantly to regional cancer rate variations across the United States. Industries concentrated in specific geographic regions create localised patterns of occupational cancer risk that manifest in state-level cancer statistics. Mining, petrochemical production, agriculture, and manufacturing industries each present distinct carcinogenic exposure profiles that affect worker populations and surrounding communities.
Historical occupational exposures continue to influence current cancer patterns due to the long latency periods associated with many occupational carcinogens. Asbestos exposure from shipbuilding, construction, and manufacturing industries during the mid-20th century continues to generate mesothelioma and lung cancer cases decades after initial exposure. Similarly, benzene exposures in petroleum and chemical industries create persistent leukaemia risks that may not manifest until years or decades after occupational contact.
Regulatory improvements in workplace safety standards have reduced many occupational cancer risks, but legacy exposures and ongoing hazards in certain industries maintain elevated cancer burdens in affected regions. The cumulative impact of multiple occupational carcinogens in industrial communities creates cancer risks that extend beyond individual workplace exposures to affect entire regional populations through environmental contamination and community-wide exposure pathways.
Asbestos exposure in construction industry workers
Asbestos-related cancers, including mesothelioma and lung cancer, continue to affect construction workers and their communities decades after peak asbestos use periods. States with extensive construction and renovation activities, particularly involving older buildings constructed before asbestos regulations, face ongoing occupational exposure risks. Demolition and renovation projects in industrial states like Pennsylvania, Ohio, and Michigan generate continued asbestos exposure potential for construction workers and nearby residents.
Shipyard workers in coastal states experienced particularly intense asbestos exposures during World War II and subsequent decades, creating persistent mesothelioma clusters in port communities. Virginia, Louisiana, and other states with major shipbuilding activities continue to report elevated mesothelioma rates reflecting these historical exposures. Family members of asbestos workers also face increased cancer risks due to secondary exposure from work clothing and equipment , extending occupational cancer impacts beyond the immediate workforce.
Benzene-related leukaemia in petroleum refinery states
Petroleum refining operations concentrated in Texas, Louisiana, California, and other oil-producing states create occupational benzene exposure risks for refinery workers and surrounding communities. Benzene, a known human carcinogen, causes acute myeloid leukaemia and other blood cancers through bone marrow toxicity. Refinery emissions and accidental releases contribute to community-wide benzene exposures that extend occupational risks to nearby residential populations.
Epidemiological studies of refinery communities have documented elevated leukaemia rates, particularly among children living near major petrochemical facilities. The latency period for benzene-related cancers ranges from several years to decades, meaning current cancer patterns reflect both historical and ongoing exposure scenarios. Improved emission controls and workplace safety measures have reduced benzene exposures, but legacy contamination and continued low-level releases maintain persistent cancer risks in petroleum-producing regions.
Silica dust inhalation risks in mining communities
Crystalline silica exposure from mining operations creates significant lung cancer risks
for underground miners and surface workers across coal-producing states. West Virginia, Kentucky, Pennsylvania, and other mining regions report elevated lung cancer rates that correlate with silica dust exposure patterns. Silicosis, a progressive lung disease caused by silica inhalation, significantly increases lung cancer risk and creates compounding respiratory health challenges for affected workers.
The interaction between silica exposure and smoking creates particularly severe lung cancer risks in mining communities where tobacco use rates exceed national averages. Miners who smoke face lung cancer risks that are multiplicative rather than simply additive when combined with occupational silica exposure, highlighting the importance of comprehensive prevention strategies addressing both occupational and lifestyle risk factors. Surface mining operations and sand mining activities also generate substantial silica dust exposures that extend beyond traditional underground mining populations.
Formaldehyde exposure in manufacturing sectors
Manufacturing industries concentrated in states like Ohio, Michigan, and Pennsylvania create occupational formaldehyde exposure risks through wood processing, textile production, and chemical manufacturing operations. Formaldehyde, classified as a human carcinogen, causes nasopharyngeal cancer and leukemia through chronic inhalation exposures. Workers in furniture manufacturing, plywood production, and chemical processing facilities face elevated exposure risks during routine production activities.
Automotive manufacturing regions experience formaldehyde exposures through adhesive applications, composite material processing, and various manufacturing processes. The geographic concentration of automotive and related manufacturing industries in the Rust Belt creates localised patterns of formaldehyde exposure that contribute to regional cancer burdens. Improved ventilation systems and alternative chemical processes have reduced workplace exposures, but legacy health impacts continue to manifest in current cancer statistics for these industrial communities.
Healthcare infrastructure capacity and cancer treatment accessibility
Healthcare infrastructure capacity varies dramatically between states with high and low cancer incidence rates, creating disparities in both prevention and treatment outcomes. States with elevated cancer rates often struggle with healthcare provider shortages, limited specialised oncology services, and inadequate screening programme infrastructure. Rural areas within high-cancer-rate states face particular challenges accessing comprehensive cancer care due to geographic barriers and provider distribution patterns.
The National Cancer Institute designates comprehensive cancer centres and clinical research facilities primarily in major metropolitan areas, leaving rural and economically disadvantaged regions with limited access to cutting-edge treatments and clinical trials. Kentucky, West Virginia, and Mississippi have fewer NCI-designated cancer centres per capita compared to states with lower cancer incidence rates, potentially contributing to delayed diagnosis and suboptimal treatment outcomes. Travel distances to specialised care can exceed 200 miles for residents in rural areas of these states.
Medicaid expansion decisions significantly impact cancer care accessibility in high-incidence states. States that expanded Medicaid under the Affordable Care Act demonstrate improved cancer screening rates and earlier-stage diagnoses compared to non-expansion states. The correlation between healthcare policy decisions and cancer outcomes highlights the importance of healthcare access in addressing regional cancer disparities. Insurance coverage gaps particularly affect working-age adults who may delay seeking care for symptoms or skip recommended screening procedures.
Healthcare workforce shortages compound infrastructure limitations in high-cancer-rate states. Oncology nurse shortages, radiation therapy technologist availability, and medical oncologist distribution patterns all affect cancer care delivery capacity. States with challenging economic conditions and limited educational opportunities struggle to attract and retain healthcare professionals, creating persistent gaps in cancer care capability. Telemedicine initiatives and mobile health programmes offer potential solutions for extending specialised care to underserved areas, though implementation requires substantial technological infrastructure investments.
The intersection of cancer incidence patterns and healthcare infrastructure capacity creates feedback loops where states with the greatest cancer burdens may have the least capacity to address these challenges effectively.
Cancer treatment facility capacity measurements reveal significant disparities between high and low-incidence states. Radiation therapy equipment availability, chemotherapy infusion capacity, and surgical oncology services all show geographic concentration patterns that favour urban areas in states with better overall health infrastructure. These capacity limitations can result in treatment delays, compromised care quality, and worse survival outcomes for patients in underserved regions. The geographic maldistribution of cancer care resources perpetuates health disparities and may contribute to the persistence of regional cancer rate differences across the United States.